Training better doctors and training doctors better | Reflections of a medical educator | Aiming to improve medicine, one blog post at a time | Also a place to put my family history research | Reach out via Twitter @drandrewhuang
Writing up my results – Learning from exemplars in Qualitative research
At my last PhD supervision meeting, the document I submitted for revision was undercooked. It was a big data dump of some my participant quotes without much synthesis by me. Out of this, I was given the homework of reviewing three authors to see how they wove participant quotes into their results. I’ll be looking at these three papers, especially how they used participant quotes:
LaDonna, Kori A., Lindsay Cowley, Claire Touchie, Vicki R. LeBlanc, and Edward G. Spilg. ‘Wrestling With the Invincibility Myth: Exploring Physicians’ Resistance to Wellness and Resilience-Building Interventions’. Academic Medicine 97, no. 3 (March 2022): 436–43. https://doi.org/10.1097/ACM.0000000000004354.
Castanelli, Damian J, Jennifer M Weller, Anusha R Chander, Elizabeth K Molloy, and Margaret L Bearman. ‘A Balancing Act: The Supervisor of Training Role in Anaesthesia Education’. Anaesthesia and Intensive Care 47, no. 4 (1 July 2019): 349–56. https://doi.org/10.1177/0310057X19853593.
Watling, Christopher, David Sandomierski, Sophie Poinar, Jennifer Shaw, and Kori LaDonna. ‘The Courage to Advocate: How Two Professions Approach Public Advocacy Work’. Medical Education n/a, no. n/a. Accessed 13 June 2024. https://doi.org/10.1111/medu.15430.
I’ll also draw on Braun and Clarke’s book.
LaDonna et al
First paragraph of the results used a number of quotations in line with the text:
“When asked about burnout and strategies intended to enhance their wellness and boost their resilience, participants responded with a range of emotions. Many were frustrated, some expressed irritation, and a few became angry. Although not all participants endorsed feeling burnt out, most characterized the work of a physician as a seemingly never-ending cycle of “managing crisis, then another crisis, then another crisis” (Participant 3 [P3]) in a health care system beset by limited resources. And while being in a constant state of high alert and having to “do more with less” (P18) certainly caused stress, participants perceived that these were not the primary causes of burnout. Rather, while they often felt overworked, participants perceived that physicians had the constitution and training to withstand stress because “we were selected to be this way. There is no amount of challenge that would faze us” (P6). Instead, a perceived inability to overcome pervasive and problematic organizational and professional values seemed to be both the biggest threat to their well-being and the source of resistance to strategies aimed at enhancing it. We will expand on each of these findings using illustrative quotations (labeled with the participant identification number in parentheses).”
LaDonna et al here are using the participants words to help build LaDonna’s own narrative. The quotations here are small excerpts of the participants words that are descriptive.
The next section is a theme “Wrestling with the invincibility myth” developed using constructivist grounded theory:
Although most participants stated that they loved the work of doctoring, they felt that the medical profession was moving away from the values of caring and compassion that initially inspired them to become physicians. Instead, they perceived that medicine’s organizational and professional values have “become flow, capacity, throughput, budgetary, meeting targets. We’ve moved very much away from caring for the patient….” (P13). This shift has created a culture of busyness and “achievement [where] you’re valued for what you can bring to the organization, the prestige, the amount of work, the sheer volume of work that you can do” (P6).
Here in this paragraph, KaDonna opens with an insight/interpretation. She then provides some patient voice that supports the interpretation. This is the “what”. Following this she goes to the “so what”. What: Doctors love their work but feel like cogs in a machine. So what: that is created a suboptimal culture.
For participants, engaging in overwork and constantly striving to excel were rewarded by their organization and perceived as virtuous: The later you stay … the more that you’re doing, well, clearly then you’re a better doctor. You’re more likely to be promoted … you’re a better person all around, not just a better doctor, but a better person because you’re committed and you’re willing to sacrifice everything for medicine. (P4)
What: if you overwork you’re rewarded, then using a participant quote to illustrate.
Several participants spontaneously characterized this constant striving as a vestige of an invincibility myth or “the old way of thinking, that doctors viewed themselves as invincible … because they had the answer to everything, they were the keeper of all knowledge. And they could heal you” (P5). The invincibility myth was evident in what participants perceived as unrealistic expectations for both their work performance and personal behaviors. For instance, because medicine is a high-stakes profession, participants perceived zero margin for error: A lot of physicians have a tendency to expect themselves to make no mistakes … it’s so unrealistic…. You try the best you can to do everything right; it’s just impossible that you can be a hundred percent all the time. (P9)
What: This culture is typical of the invincibility myth. Then another illustrative quote.
Also implicit within the invincibility myth was the message that “it’s always work first…. You’re not supposed to have any weakness” (P4), causing several participants to use words like “superhero” (P19) and “superhuman” (P4, P19) to describe how physicians were both outwardly perceived and internally enculturated to behave as invincible: “Some generations feel like they’re superhumans or superheroes. That they can conquer the world, you know, they can have no sleep, they don’t need to eat….” (P19).
What: Doctors think they need to be superhuman or superheroes.
Because of these entrenched professional values, participants described feeling pressured to prioritize their professional obligations over their personal lives and physical needs. Consequently, taking time off for illness, vacation, or family reasons was perceived as a countercultural act for which they were punished: It’s the culture … it doesn’t take into account how busy and stressed people need their vacation…. A lot of people have expressed the idea of makeup clinics [suggesting] that we are being punished for taking vacation…. We are asked to do more to make up for the fact that we’re away. (P10)
What: The culture means doctors prioritise their professional oblications over personal needs. So what: Time off was punished.
Additionally, in a work culture that assumes invincibility, even the very human experience of being sick was perceived as inconceivable, not only because physicians are supposed to be superhuman but also because they perceived their absence would create problems for both their patients and their colleagues: It’s not really acceptable to be sick…. If I’m sick and I don’t show up in the morning, then someone has to cancel 27 patients … all these patients don’t know what to do or who will take care of them…. (P16)
What: It’s unacceptable to be sick because of this culture.
In turn, living up to the standards of the profession created an uncomfortable tension between being human and being professional—even in the face of workplace stress or bullying from patients or colleagues: You’re supposed to be this person who never gets rattled, who gets called to an emergency, [to] handle it and listen to someone shouting at you for no reason and be able to take it and not get upset. Which is a human thing to do is to be upset. Right? But you’re not allowed to as a physician … it’s human but it’s not professional … you have to really learn, as a physician, to hold your feelings in. (P14)
So what: there is a tension between being the professional facade and your natural emotions. Then a quote to illustrate.
Reflecting on the way LaDonna is using the participant quotes, she’s using the indented parts for 3-5 sentences at the end of a claim to support or illustrate the claim she’s making.
Castanelli et al
Castanelli et al’s article uses Thematic analysis, so might be more applicable to my study. Let’s see how he uses participant quotes.
The opening to the results section has an introductory paragraph:
We ceased interviewing after 19 interviews, when we judged the thematic structure sufficient to address the research questions, as described by Braun and Clark.10 We interviewed eight male and 11 female participants and the median experience in the role was four years (range one to 11 years). Four participants were from New Zealand, with at least one from each Australian state and territory. Four participants came from each of small metropolitan, large regional and small regional hospitals, whereas seven participants were from large metropolitan hospitals.
The first paragraph here is the demographics of the population that was interviewed.
We identified four themes in our analysis of the Supervisor of Training role. In the first three themes, the Supervisors of Training described themselves as ‘the something in between’, balancing competing interests. We observed that participants perceived themselves as the fulcrum of the learning environment in their workplace. In this shared view of their role, they reported facilitating the key relationships between all those involved in training. They used many similar expressions such as ‘lynchpin’, ‘interface’, ‘go-to person’, or ‘go-between’ to describe this fundamental conception of their role. In maintaining their place as the fulcrum of the learning environment, we observed that Supervisors of Training needed to make constant adjustments and accommodations to balance competing interests and responsibilities; they perceived themselves to be representing trainees, colleagues, their hospital, ANZCA and the community to varying degrees at different times. Negotiating these competing responsibilities required managing multiple different relationships and entailed a significant amount of emotional work. Our fourth theme described the imbalance between the demands of these first three themes and the preparation and resources available to our participants.
The four themes we identified were: 1. Guiding and assessing trainees. 2. Identifying, supporting and adjudicating trainee underperformance. 3. Mediating trainees’ relationship with the hospital. 4. Scarcity: inadequate orientation, support and time.
In this paragraph, Castanelli provides an overview of what he is about to spell out in the themes. Let’s look at the first theme
The Supervisors of Training’s interaction with trainees entailed two potentially discordant functions: guidance and assessment. For the most part, Supervisors of Training saw themselves primarily as ‘a guide, assisting trainees to understand what they need to do and helping them navigate ANZCA training’ (Participant 3). Guiding trainees was seen as a continuous process that followed a rhythm of planning, interim and feedback interviews with trainees across their placement that provided the scaffolding for this assistance. There was a particular focus among Supervisors of Training on keeping trainees aware of the ANZCA training requirements and the need to record these in their electronic portfolio.
What: how Castanelli interpreted the SOTs as guiding and assessing. Uses a quotatio as part of the narrative. Then expands on what this means.
For Supervisors of Training, the electronic portfolio required ‘a very large amount of documentation and administrative stuff’, which was seen as necessary to ensure a ‘robust and clearly documented training scheme’ (Participant 6). However, this entailed a significant opportunity cost in that it decreased the time available for meaningful interaction with trainees: ‘I’m spending a significant amount of time in front of the computer going through paperwork’ (Participant 17). At the extreme, this created the perception the Supervisor of Training had become ‘essentially a bureaucrat: tick the boxes, make sure the boxes continue being ticked’ (Participant 1).
What: SOTs did lots of admin. This resulted in lost opportunity costs (all supported by in-line quotes.)
Despite the prominence of routine bureaucratic duties, Supervisors of Training reported their guidance extended beyond assistance with meeting administrative requirements. They saw themselves as integral to supporting trainees’ self-directed learning: ‘Helping them to develop skills in order to be competent anaesthetists at the end and guiding them to do that. Where they have weaknesses, just helping them to identify what those are and providing them with opportunities to assist them to improve in those areas.’ (Participant 3)
This is a so what (not just bureacracy, but also as a support) paragraph, supported by a more extended quotation.
The guidance aspect of the role for some participants involved a pastoral component, providing ‘a port of call for welfare issues’ (Participant 11). Participants also reported providing career advice that gave a future orientation to their support for trainees, where they aimed to: ‘Look after a trainee through their journey, not just through their rotation with us.’ (Participant 16)
What: SOTs saw a pastoral care element to their role (with quote)
A competing yet equally fundamental aspect of the Supervisor of Training role for all participants was assessing trainee performance. Our participants saw themselves as collectively responsible for ensuring graduating specialist anaesthetists were appropriately qualified for their work. This collective responsibility was expressed both as a duty to the profession and the community, for example: ‘I have a responsibility to the public to ensure that (trainees) are of sufficient standard that they can do their job safely.’ (Participant 3)
What: there was also an element of assessment (with quote)
Supervisors of Training recognised the conflict inherent in their dual responsibility for both assessing and guiding trainee learning: ‘We try and separate out the assessment role from the supportive role, but you end up doing both of course.’ (Participant 12)
What: SOTs recognised different aspects.
Some participants thought it was inevitable that they would be seen as ‘gatekeepers’ (Participant 19) once a trainee’s performance was in question, whereas others were reluctant to be the ‘policeman’ (Participant 3). One way of managing this conflict reported by experienced Supervisors of Training was to ‘get the trainee to see that we care about your training’ (Participant 16) and emphasise their role in helping the trainee deal with questions about their performance ‘because we want you to improve, to become a better anaesthetist’ (Participant 16).
Here Castanelli is using in-line quotations to explain the phenomenon.
Watling et al.
We found that public advocacy occurs at the intersection of personal and professional identities. Those who engage in public advocacy appear attuned to social injustice and gaps in systems that may cause harm if not addressed. Their work is facilitated by personal courage and exposes them to personal and professional risk. Comparing professions, we found variability in how participants positioned themselves as advocates and how they positioned their advocacy work with respect to their professional identity. Some (more often lawyers) placed advocacy firmly within their professional role, while others (more often doctors) positioned it outside of their professional role. All participants drew on their professional background and training to advance their work, which created both opportunities and blind spots. Below, we elaborate these ideas and illustrate them with representative quotations from participants.
In this opening paragraph, Watling et al use no quotation. They outlined their themes without explicitly naming them – addressing inequality; summoning courage; leveraging privilege; embracing an advocate identity, and; drawing on skill, attitudes and evidence. Or perhaps they named them but used shorter titles as headers. Each of these titles is short and uses the participle rather than making a statement.
In both professions, we found people were drawn to public advocacy by a sensitivity to perceived injustice. For some participants, this orientation predated their professional training; one lawyer noted that even before law school, “I’ve always been drawn to social justice stuff” (P12, lawyer), while another participant referenced their upbringing as nurturing their advocacy: “When I perceive inequity, in particular racism, or unreasonable behavior that is unfair and biased, I personally have been raised never to tolerate it.” (P9, MD/lawyer). For others, this sensitivity was heightened by frustrations experienced in their professional practice; one physician noted that “there’s huge gaps where we don’t serve patients” (P5, MD). Others were attuned to those left behind by existing systems: “We were seeing kind of a disproportionately privileged group of people, and that people who had confidence speaking up for themselves would be more readily accessing care. And I was kind of wondering who we were not seeing.” (P15, MD). For still others, the sense of injustice was felt at a societal level rather than a professional practice level; one lawyer participant was drawn to advocacy work because “I don’t think we have the rights we need in the [Canadian] Charter of Rights” (P1, lawyer). Public advocacy, therefore, was for almost all participants a means of trying to close gaps, to improve access to health care or access to justice and to address inequities.
Watling et al here are very succinct. They make a claim about public advocacy, start quoting in-line to justify their claim; rinse and repeat. They then close the paragraph with a summarising “so what” sentence.
Reflection: There is a certain amount of confidence that the authors exude when writing here. They say something, back it up with a small amount of data, then move onto the next point.
Braun and Clarke on interpretation and using quotes
Braun and Clarke’s book actually outlines how to write up a thematic analysis in chapter 5. (I’ve previously blogged about chapter 4 here.) Here are some snippets of advice they give:
the purpose is to tell a story. “What you’re doing in this section is providing the reader with examples of what you claim the data evidenced and what you think the patternings mean. Your data must be interpreted and connected to your broader research questions, and to the scholarly fields your work is situated within.”
write an introductory overview. This can be done as a list, a table, or a figure. Just be mindful not to present things as a topic summary (there needs to be a degree of synthesis or interpretation)
“We very loosely recommend a 50–50 balance of these two aspects (data extracts and analytic narrative): not too much data to suggest the analytic narrative aspect is underdeveloped”
Braun and Clarke prefer to combine results and discussion in an “analysis section. But where you have to separate the two, they suggest one of two methods: reporing the the themes in a more descriptive way; or develop a more interpretive account and expand with reference to other literature in the discussion. (See box 5.4)
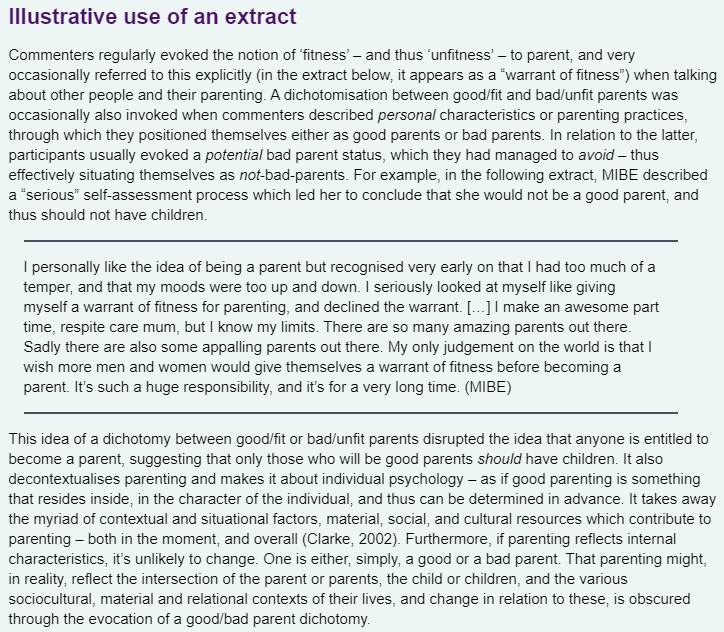
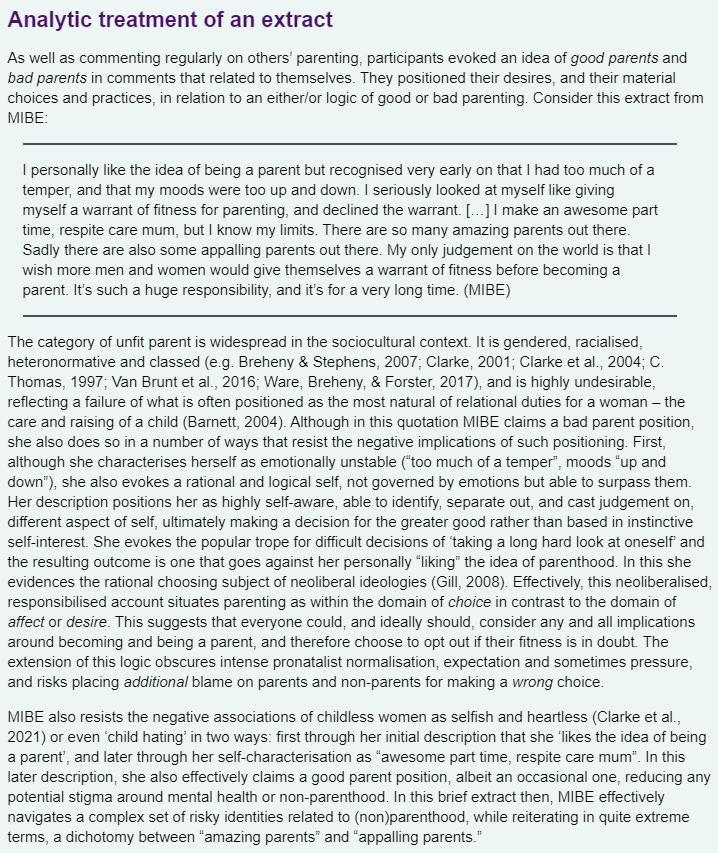
This is from box 5.5 illustrating two different ways of using the same quote.
Here you can see then the analytic treatment is given to the text, there is more interpretation with two long paragraphs following the quote, whereas the more descriptive version is closer to the 50:50 balance. Both versions have a what, quote to illustrate the what, then so what format.
Trap – don’t just paraphrase the illustrative quote in the “so what section”
Consider “thick descriptive” techniques – often these techniques help add nuance and context to the quote.
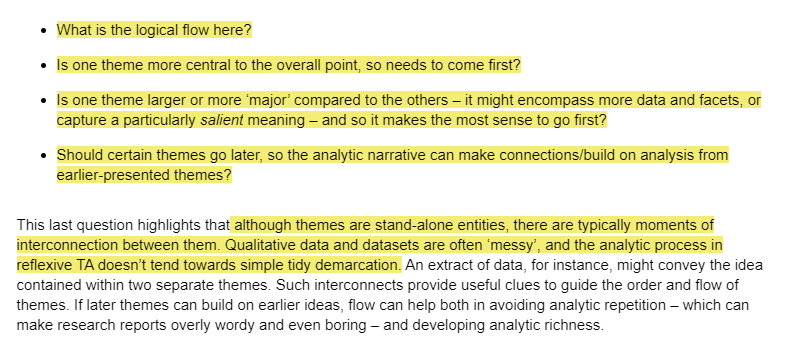
Consider the flow of the story – “which theme best comes first, to tell the best story?”
be aware of the spectre of “generalisability”. Think more in terms of “transferability” and whether the story resonates to others working in related fields.
Braun and Clarke have a section in the book titled “drawing conclusions”. I see this as the answer to “so what?” and “now what?”
After it’s all done, critically reflect and edit, edit, edit to refine the story.
They recommend two books to refine your craft:
Conclusion
I think I’m ready to revisit this results section. I need to keep in mind – what’s the story I’m trying to tell? I also need to tell it in my own voice but with participant quotes to support my analysis.