This morning there weren't enough nursing staff to run the theatre I was allocated to this morning. In addition one of the fellows was sick after having a Covid vaccination. I was redeployed to his theatre to help a colleague of mine doing a paediatric ENT list. 1/
We turned it into a peer review session for my colleague. One of the comments that he made was that he prefered to use TIVA for kids- he had used paedfusors for about 4 years in Cambridge. However, we don't have the equipment in our institution and so he defaulted to sevoflurane.
I had never used the paedfusor when I trained at the Sydney Children's Hospital, nor had I ever used it in any of the paediatric cases during my training.
But I converted to fully TIVA in 2013. This is a thread on my hack for propofol TIVA in kids without having a paedfusor. 3/
These are the teaching slides I put together about it. They also act as a reminder for me for when I do any paediatric cases.
This slide is based on Mani, Vaithianadan, and Neil S. Morton. ‘Overview of Total Intravenous Anesthesia in Children’. Pediatric Anesthesia 20, no. 3 (2010): 211–22. https://doi.org/10.1111/j.1460-9592.2009.03112.x.
4/

This is the source material from Mani and Morton. 5/

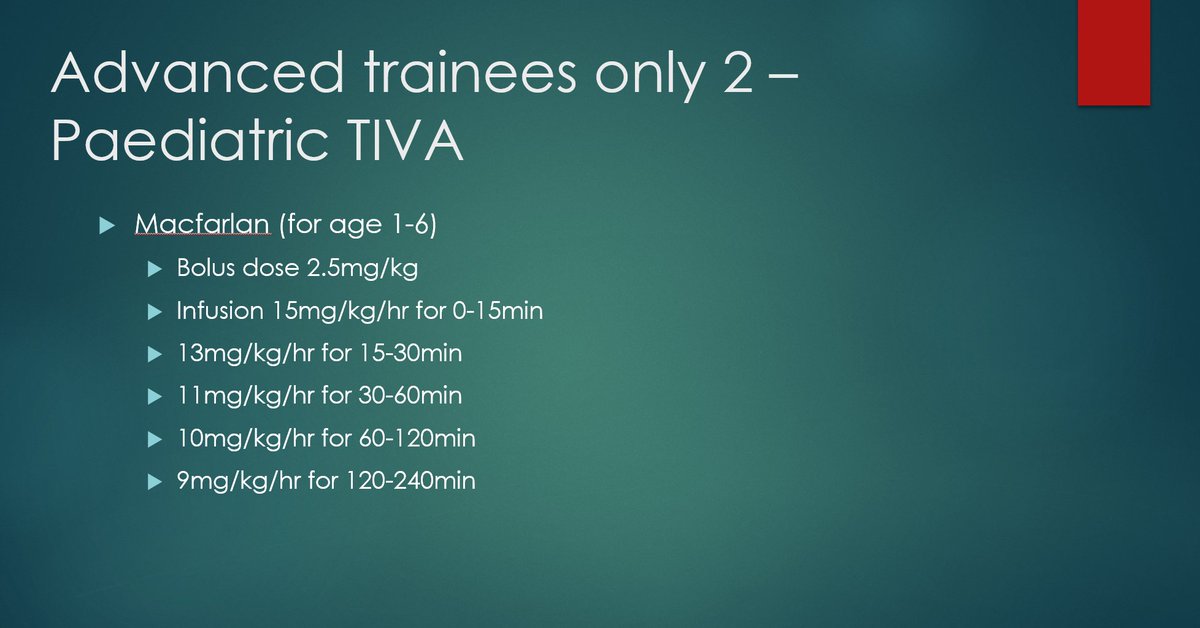
The same article cites the Macfarlan model too. 6/

And here is my slide. I started putting the slides together probably around 2015 (I found myself parroting the same thing list after list), and I haven't really touched them much since 2017. I've also moved away from didactic imposition of knowledge. 7/
But in my experience I'd normally be aiming for a higher propofol concentration.
I thought the low 1mg/kg loading dose of Roberts/Paedfusor was too low and preferred the 2.5mg/kg used in the Macfarlane model. 8/

So my cookbook recipe involves:
1. Taking the Macfarlan loading dose
2. Increasing the paedfusor stage 1 dose by 50% (from 19-30mg/kg/hr) to initiate anaesthesia and ensure the patient is asleep
3. Increasing paedfusor stage 2 dose by 50% from 15-22mg/kg/hr
9/

4. Increasing paedfusor stage 3 dose by 50% from 12 to 18mg/kg/hr.
I hope by doing that I'm approximating a plasma concentration >3.0mcg/ml (and closer to 4.5mcg/ml).
10/

I'm sure there are errors in my logic and it doesn't fit the compartment model, but this "Huang hybrid" model has worked for me over the years.😂
And note when the kids are adult size (40+kg), I just use the Schnider model.
@GongGasGirl @scruff888
11/11
Originally tweeted by Dr Andrew Huang 黄延祺 (@DrAndrewHuang) on November 23, 2022.

One thought on “Paediatric Profofol TIVA without a Paedfusor”